Endometriosis Mimicking Ovarian Cancer: Advanced Surgical Management
Understanding Endometriosis Mimicking Ovarian Cancer
Introduction
Endometriosis is a common gynecological condition in which tissue similar to the lining of the uterus grows outside the uterus. While many patients experience pelvic pain or infertility, severe endometriosis can sometimes mimic advanced ovarian cancer on imaging and clinical evaluation.
At Naman Cancer Clinic & Research Centre, we recently managed a challenging case where extensive endometriosis closely resembled carcinoma ovary both clinically and radiologically, requiring major multi-organ surgery and careful intraoperative decision-making.
Case Summary
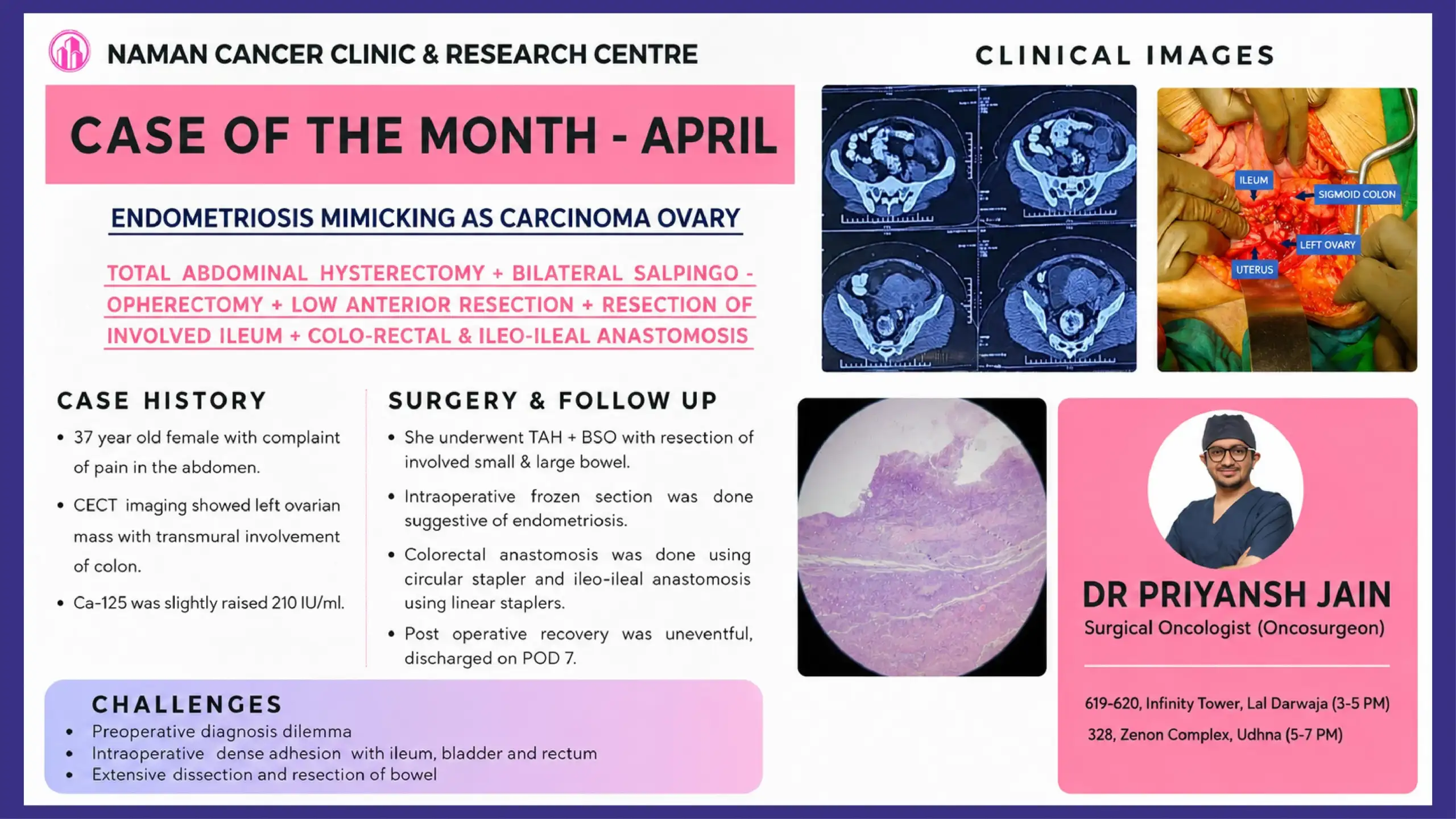
A 37-year-old female presented with complaints of persistent abdominal pain. Further evaluation with Contrast Enhanced CT (CECT) imaging revealed a left ovarian mass with transmural involvement of the colon, raising strong suspicion for ovarian malignancy.
Tumour marker evaluation showed mildly elevated CA-125 levels of 210 IU/ml, which further added to the diagnostic dilemma.
Based on imaging findings and the extent of disease involvement, the possibility of advanced ovarian cancer was strongly considered.
Why Endometriosis Can Mimic Ovarian Cancer
Severe endometriosis can occasionally behave like a malignant disease because it may:
- Form large pelvic masses
- Cause dense adhesions between organs
- Invade surrounding bowel or bladder
- Elevate CA-125 levels
- Produce extensive fibrosis and inflammation
These findings can appear very similar to ovarian cancer on CT scans and during surgery.
This overlap often makes definitive diagnosis difficult before surgery.
Surgical Procedure Performed
Considering the extensive pelvic disease, the patient underwent:
- Total Abdominal Hysterectomy (TAH)
- Bilateral Salpingo-Oophorectomy (BSO)
- Low Anterior Resection
- Resection of involved ileum
- Colo-rectal anastomosis
- Ileo-ileal anastomosis
The surgery required extensive pelvic dissection due to severe adhesions involving:
- Ileum
- Sigmoid colon
- Rectum
- Bladder
- Left ovary and uterus
Major Surgical Challenges
1. Preoperative Diagnostic Dilemma
The biggest challenge was differentiating severe endometriosis from ovarian cancer before surgery.
The imaging findings, bowel involvement, and raised CA-125 strongly suggested malignancy.
2. Dense Pelvic Adhesions
Intraoperatively, there were extensive adhesions between pelvic organs, making dissection technically demanding and increasing the risk of bowel or urinary tract injury.
3. Multi-Organ Involvement
The disease involved both small and large bowel, requiring bowel resections and reconstruction.
Role of Frozen Section
An intraoperative frozen section analysis was performed during surgery.
Surprisingly, the frozen section was suggestive of endometriosis rather than malignancy.
This was a crucial turning point in surgical decision-making, helping tailor the extent of surgery appropriately and avoid unnecessary radical oncological procedures.
Bowel Reconstruction
After resection of the diseased bowel segments:
- Colo-rectal anastomosis was performed using a circular stapler
- Ileo-ileal anastomosis was completed using linear staplers
Careful reconstruction ensured restoration of bowel continuity and function.
Postoperative Recovery
The patient had an uneventful postoperative recovery and was discharged in stable condition on Postoperative Day 7.
This case highlights the importance of multidisciplinary planning, surgical expertise, and intraoperative pathology support in managing complex pelvic masses.
Understanding Deep Infiltrating Endometriosis
Deep infiltrating endometriosis is an aggressive form of endometriosis that extends beyond superficial pelvic tissue and may involve:
- Bowel
- Bladder
- Ureters
- Pelvic nerves
Symptoms may include:
- Severe pelvic pain
- Painful menstruation
- Pain during bowel movements
- Infertility
- Abdominal bloating
In advanced cases, surgery becomes necessary to relieve symptoms and remove affected organs or bowel segments.
Key Learning Points
- Endometriosis can closely mimic ovarian cancer clinically and radiologically.
- CA-125 elevation is not specific for ovarian malignancy.
- Frozen section analysis plays a critical role in difficult pelvic masses.
- Advanced endometriosis may require complex bowel surgery.
- Multidisciplinary surgical planning is essential for optimal outcomes.
Conclusion
This case demonstrates how severe endometriosis can present as a complex pelvic mass resembling advanced ovarian cancer. Accurate diagnosis, careful intraoperative assessment, and meticulous surgical management are essential to achieve good outcomes while avoiding overtreatment.
At Naman Cancer Clinic & Research Centre, we continue to manage complex oncological and oncologically mimicking conditions with evidence-based, patient-centered care and advanced surgical expertise.
Also read,
Dr Priyansh Jain
Surgical Oncologist (Oncosurgeon)
Naman Cancer Clinic & Research Centre, Surat
Also read: Bilateral VATS Surgery for Thymoma: Advanced Minimally Invasive Mediastinal Mass Removal
Also read: Advanced Oral Cancer Surgery with ALT Free Flap Reconstruction



